
The Mayo Clinic Guide to Pain Relief by Wesley P. GIlliam, Ph.D., and Bruce Sutor M.D explains how pain develops, how it can become chronic, and what you can do to free yourself from chronic pain’s effects.
There are three primary dimensions that make up the chronic pain experience: sensory, cognitive and emotional.
- The sensory dimension refers to the intensity, location and quality of the pain that you’re experiencing. This dimension relates to the biological aspects of pain, covered in the previous chapter.
- The cognitive dimension includes the thoughts that run through your mind as you try to make sense of what pain means for you now and what ongoing pain might mean for you in the future.
- The final dimension is your emotional response to pain, such as feelings of sadness, anxiety, anger and fear. These emotions motivate responses to pain that might make sense in the moment but can create long-term challenges.
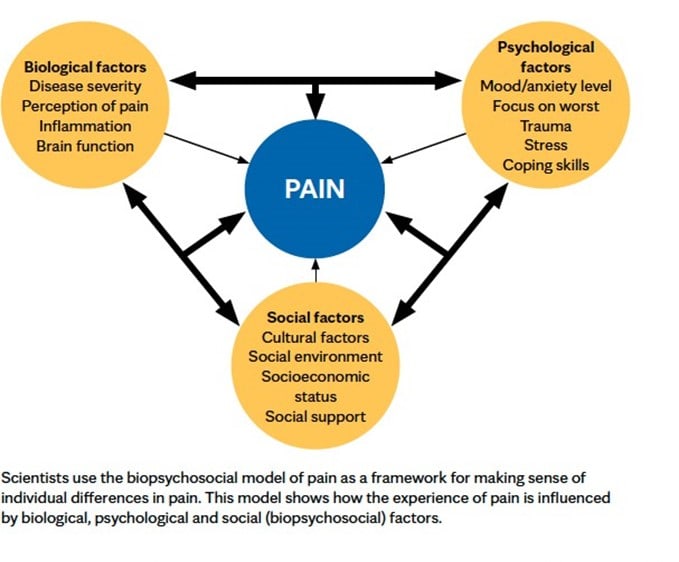
The way these three dimensions affect one another influences how your brain interprets sensory information from your body and, ultimately, your pain response. The cognitive and emotional factors that contribute to the pain experience are often referred to as psychosocial factors.
The Power of Thoughts and Emotions
Remember how sensitization can amplify pain, like having the volume control on a radio stuck on high? In a similar way, thinking negative thoughts and experiencing negative emotions can amplify pain and make things hurt more.
The opposite is also true – more balanced, positive thoughts and emotions can turn down the pain volume. This can be hard to imagine in the context of pain, but a person’s thoughts and emotions – the psychosocial factors – are some of the best predictors of how well someone will function with chronic pain.
Extensive research shows that certain psychosocial factors contribute significantly to the negative effects of chronic pain.
Depression
Chronic pain and depression often go hand in hand. Depression is more common in people with chronic pain than in those who don’t have chronic pain. At the same time, experiencing depression puts people at higher risk of developing chronic pain.
Research shows that people who are initially pain-free but have severe depression are about four times more likely to develop pain 12 months later when compared to people with no depression. Similarly, people with pain are twice as likely to develop depression 12 months later when compared to people with no pain. This suggests that chronic pain and depression are risk factors for each other.
It’s natural to experience some discouragement when pain first develops and for a short time after. The pain itself can cause slowed movements or loss of energy, symptoms often associated with depression. If your symptoms linger for several weeks or they become severe, it’s an indication that you may be experiencing depression. If this happens, it’s important that you talk to a medical professional.
Treatment for depression is often very effective. And it can result in less pain or pain that’s easier to manage.
Anxiety
Anxiety is a feeling of fear or worry.When people experience chronic pain, they can become overly anxious about their pain over time. This fear can make a person focus more on the pain, making it feel worse.
Like depression and chronic pain, high levels of anxiety can predict the risk of developing pain, whereas chronic pain can increase the likelihood of anxiety. Interestingly, research shows that the brain areas activated by chronic pain and anxiety overlap.
Sometimes pain-related anxiety becomes so great that it makes a person avoid movement for fear that it will hurt. This is known as kinesophobia, a fear of movement that typically leads to decreased physical activity. As activity decreases, the body becomes weaker, which leads to greater susceptibility to pain.
Anger
Anger is another common emotion associated with chronic pain. It’s not surprising that when something hurts, you feel irritable. Most people with chronic pain report feeling angry at themselves or at others on a consistent basis. Among people with chronic pain, high levels of anger or irritability are often associated with greater muscle tension and pain severity.
While feeling angry can contribute to increased pain, just as important is how anger is expressed. Research has shown that actively trying to suppress or hide anger results in increased muscle tension, specifically around the painful area — which only increases the intensity of the pain. On the other hand, certain outward expressions of anger, such as shouting or becoming physically agitated, also can result in greater pain.
Catastrophic thinking
As chronic pain sets in and starts to negatively impact numerous areas of life, this struggle can begin to change how people think about pain, about themselves and about others around them.
Thoughts are incredibly powerful. For some people with chronic pain, just thinking of a particular movement or watching someone else perform that movement can produce very real pain. There’s even evidence to suggest that simply imagining movements associated with the area of chronic pain can result in swelling of the painful area. Is this real pain? Yes.
Negative thoughts such as “I’m in pain, so there must be something wrong with me” and “I’ll never be the person I used to be until this pain goes away” can keep pain active and even make it worse. They can make people anxious about their pain and any activity associated with it. In fact, anticipating the worst possible outcome, or catastrophizing, activates pain pathways in the brain and can create pain experiences.
Pain catastrophizing is a way of thinking that views the experience of pain as uncontrollable, permanent and destructive. People who tend to interpret their pain in catastrophic ways are prone to becoming preoccupied by their pain. They have a difficult time distancing themselves from their pain, and so they spend excessive amounts of time thinking about their symptoms.
Catastrophic thinking also tends to magnify the pain experience. That is, as you spend more and more time thinking about pain, it begins to take up more of your life. Along with this change often comes a sense of helplessness. Nearly 30 years of research have shown the negative effects catastrophic thinking has on pain, as well as on your overall health and well-being. And pain catastrophizingis related to depression, anxiety and anger.
The Pain Response
How a person responds to pain is an important consideration in pain management. Responses to pain are influenced by your thoughts — your interpretation of the meaning of pain — and the emotions you experience.
One way to respond to pain is to avoid activities that are painful. In some cases, it is better to avoid certain activities as part of a healthy pain management approach. For example, if you have chronic knee pain, taking up running again might not be the best idea. But that doesn’t mean all physical activity is unsafe; it just means certain activities might not be in your best interest anymore.
Caught in a Cycle
As negative thinking patterns and emotions around chronic pain become stronger, worry about pain can lead to increased avoidance of activity — not just physical activities but also social and work-related activities.
The thing is that human bodies are made to move. Inactivity can make your body weak — a process called physical deconditioning. A deconditioned body is more susceptible to experiencing pain, which feeds into more negative thinking and fear, all of which contribute to a more sensitive pain alarm in the brain. An overly sensitive pain alarm can trigger unhealthy behavioral patterns in response to pain. These are called pain behaviors.
Pain behaviors
Pain behaviors are intended to ease the experience of pain in the moment but often serve to maintain pain and related symptoms in the long term. Some common pain behaviors include limping, groaning, limiting activity, staying in bed for extended periods of time and isolation.
These behaviors also can influence the reactions of others. For example, the frequency with which a loved one expresses sympathy or offers unnecessary assistance with daily tasks — also referred to as solicitous responses to pain behaviors— can actually make the situation worse. Research shows that solicitous responses from family members, especially a spouse, are associated with greater pain, worse physical functioning and increased use of healthcare among people with chronic pain.
Pain behaviors can create tension within important relationships. Some family members, friends and co-workers may get frustrated when they see repeated pain behaviors and so may respond to them in critical ways. They might say things like “Here we go again” or “I’m trying to help you but it seems nothing I do is enough.” These types of negative interactions, also called punitive interactions, can harm important relationships and create distress.
Both solicitous and punitive responses to pain behaviors can create additional focus on a person’s symptoms, which effectively worsens chronic pain.
Cultural influences
Culture is commonly defined as the set of beliefs, attitudes and customs that distinguish one group of people from another. Each of us has a unique set of cultural attributes, often brought together from a variety of sources, that influence our daily experiences. This includes experiences of pain.
Evidence shows that cultural factors may impact our sensory perception of pain, ability to tolerate pain, and beliefs about the causes of pain. Our cultural backgrounds also can impact how we communicate about pain — both nonverbally, such as through facial expressions, and verbally, such as through the words we use.
Culture plays a role in determining our expectations for how pain should be managed, such as primarily with medications and procedures, for example, or mostly with do-it-yourself strategies, such as exercise programs or relaxation techniques.
More recently, medical institutions have placed greater emphasis on training healthcare professionals to identify, consider and respect the cultural factors that may impact a person’s pain experiences.
It’s reasonable and appropriate for you to discuss with your healthcare team any cultural beliefs, attitudes or customs that have influenced your experience of pain, including symptoms, treatments and coping approaches. This approach helps your healthcare team have a more holistic view of your experiences and how pain impacts your life.
Building New Pathways
Chronic pain is an experience that changes the brain over time. The negative thoughts, emotions and behaviors discussed in this chapter — while common and understandable — can become entrenched and contribute to the development of pathways that allow the brain to easily produce pain. As a result, the brain becomes good at creating pain.
But the fact that your brain can change is also good news. Thoughts, emotions and behaviors can be rewired in your brain in a positive way. In the coming chapters, you’ll learn how you can retrain your brain to become less reactive to pain and diminish pain’s impact on your life.
Relevant reading
Mayo Clinic Guide to Fibromyalgia
Drawing on decades of experience in treating fibromyalgia, Mayo Clinic Guide to Fibromyalgia offers research-supported, practical strategies that can help anyone with fibromyalgia live their best life. From personal stories of people living with fibromyalgia to the compassionate expertise of its medical editors, this book seeks to connect with people…